The Cancer Waiting Times (CWT) standards are guidelines established to ensure timely diagnosis and treatment for cancer patients, with significant updates implemented from October 1, 2023.
The CWT standards have been streamlined from ten to three main performance standards to enhance clarity and focus on patient outcomes. These standards are as follows:
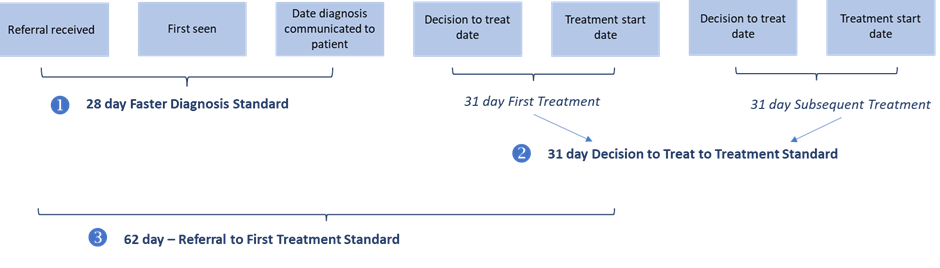
- Faster Diagnosis Standard (FDS): Patients with suspected cancer who are referred for urgent checks should receive a diagnosis or have cancer ruled out within 28 days of their referral. This aims to expedite the initial diagnostic process.
- 62-Day Treatment Standard: Patients diagnosed with cancer should start their treatment within 62 days of their referral. This standard combines previous targets for urgent suspected cancer referrals, screening, and consultant upgrades into a single measure.
- 31-Day Treatment Standard: All patients who have a cancer diagnosis and a decision made regarding their first or subsequent treatment should begin treatment within 31 days. This standard consolidates previous targets for first and subsequent treatments.
Faster Diagnosis Standard Framework (FDS)
The Faster Diagnosis Standard Framework (FDS) sets out the strategic approach to delivering faster diagnosis of cancer and the associated cancer waiting times standards.
Read more about the Faster Diagnostic Framework here
The below illustrates the Faster Diagnosis Principles which should underpin thinking, planning, review and implementation of actions for any pathway or service work.

There are key areas of focus as part of the Framework which includes:
Nationally developed best practice timed pathways (BPTPs)
We use the nationally published BPTPs to support us in developing or re-designing our cancer pathways to optimise pace of diagnosis and importantly patient experience.
As part of any pathway work or review the BPTP, where available, is used to compare best practice approach with locally designed pathways to ensure we are optimising our pathways wherever possible.
This includes looking at things such as approaches to triage, one-stop clinics and how we use our workforce most effectively at different stages of the pathway.
Non-specific Symptoms Pathways (NSS)
NSS pathways were introduced in 2020 to fill a previously un-met need to people who have symptoms suspicious of a cancer who however do not meet the NG12 criteria for a site specific suspected cancer referral.
We are committed to strengthening and sustaining the Wessex Non-Specific Symptoms pathway which is delivered by the Rapid Investigation Service, run by University Hospital Southampton on behalf of the Wessex geography.
Community Diagnostic Centres (CDCs)
The CDC programme was developed following Professor Sir Mike Richard’s review of NHS diagnostic capacity.
The vision for CDCs is to both increase and optimise capacity and access to diagnostics and improve patient outcomes and experience.
CDCs are ICB-led programmes which are required to consider and include cancer pathways as part of their overall make up of service and diagnostic offer which spans wider than cancer.
We are working closely with CDC programmes in both Dorset and HIOW systems to ensure the opportunities for development and support of cancer pathways are clearly within CDC plans.
In particular we are working together to look at opportunities to enable some of the GP direct access guidance, additional capacity for diagnostics and also to release activity on acute sites where diagnostics are clinically more appropriately delivered there.
For more information read the Medium Term Planning Framework for transforming cancer services.



Wessex Cancer Alliance Faster Diagnosis Pathway Focus 2026/27
- Complete rollout of non-medical LATP biopsy.
- Explore expansion of nurse-led cystoscopy where there are particular workforce pressures, including access to training.
- Explore opportunities to use bi parametric MRI and AI supported reporting for providers with MRI capacity challenges.
- Complete the rollout of Unscheduled Bleeding on HRT pathways.
- Explore expansion of non-medical hysteroscopist workforce where there are particular workforce capacity pressures, including access to training.
- Review and improve patient communication and preparedness for hysteroscopy, increasing options for pain management to reduce incomplete and repeat procedures.
- Complete the rollout of Breast Pain Pathways.
- Complete the rollout of Teledermatology.
- Continued implementation and benefits realisation of FIT within the Lower GI Urgent suspected cancer referral pathway.
- Review of local pathways in line with National pathway interventions drawn from NATCAN Audit Recommendations, including for patients with higher risk renal cell carcinoma (RCC) with a focus on reducing the variation in time to radical nephrectomy.
- Explore opportunities to streamline diagnostic and decision-making pathways with a focus on reducing variation in the time patients wait between diagnostic endoscopy and disease-targeted treatment.
In addition to the above national focus areas, in 26/27 we will also be supporting local pathway improvement projects focussed around Testicular, Head and Neck, and Sarcoma pathways.
Dr Richard Roope explains the 28-day faster diagnosis standard.
For patient information visit our fast track referrals page on Cancer Matters Wessex.